
Performance improvement project
Role: Lead UX Designer
Duration: 6 Months
Platform: Desktop and Tablet
Team: 1 UX Designer, 1 Product Owner, 1 Product Manager, 2 Tech Leads
OVERVIEW
abaqis is a quality and compliance software for skilled nursing and long term care facilities. Performance Improvement Projects are concentrated efforts on problems that arise in certain care areas or facilities. It involves the identification of the problem’s root cause, implementation of interventions into processes, and the determination if the interventions had a positive outcome on the problem.
Goals:
Update existing performance improvement project (PIP) feature to map closer to PDSA (Plan, Do, Study, Act) cycle format to better accommodate both post-acute and acute care setting users
Ensure updated feature can accommodate experienced users in intuitive performance improvement project creation and guide inexperienced users with clear steps and best practice guidance
Allow transparency for each user from project definition, intervention creation, and measurements to data synthesis and conclusions to cultivate a culture of buy-in from all project contributors
DISCOVERY
Research
This project began as a redesign of our current PIP feature from our legacy system to our new system with updated UI and enhancements. We began by exploring feedback and enhancement requests from our current users. Synthesis showed that the main pain point was the lack of trend analysis to allow them insight into whether their data collections were showing signs of improvement or not. Moving forward, we knew we wanted to explore easy-to-read data visualizations that dynamically updated with each data point collected by users.
It was later in the discovery process that we decided that this particular project would be a great opportunity to break in to the acute-care settings of hospitals, as PIPs are conducted in all medical care settings. This created a slight shift in our approach because this was a brand new industry for us to explore, meaning taking a step back and learning more about their culture, current use of PDSA, and accompanying pain points.
Interviews with Acute-Care Professionals
Through interviews with acute-care professionals, we learned that the culture of a hospital setting is incredibly siloed in their quality efforts. First and foremost, there are departments for each area of healthcare (neurology, oncology, radiology, etc.), and they each have their own processes that may or may not overlap with other departments. Within those departments, there are different levels of workers from frontline medical workers to front-desk or even security personnel. In this larger kind of facility, as we learned, there can be a common “finger-pointing” approach to events such as patient falls, hospital-acquired infections, urinary tract infections, etc. Our main takeaway: there’s a lack of concrete quality processes within hospitals that can create a joint effort for performance improvement.
SME Interviews
After learning about the environment within hospitals, we wanted to learn more about how performance improvement projects, or PDSA cycles, are conducted in the context of a hospital. Working with a SME, who is also a neuroscience critical nurse, we learned more about the process from start to finish.
Key takeaways:
1. The “pre-plan” of a PIP is the most important part to a successful project.
There is an entire process that happens before a team even begins to plan the project.
2. There needs to be a “champion”.
The quality manager who may call for a project’s creation may not even be a medical professional, so they need to enlist a front-line “champion” who is more familiar with current processes and can properly enlist team members
3. Community buy-in.
Every single team member must be updated on results of their efforts to feel as though their time isn’t wasted, or they will not provide efficient work.
Synthesis
Personas
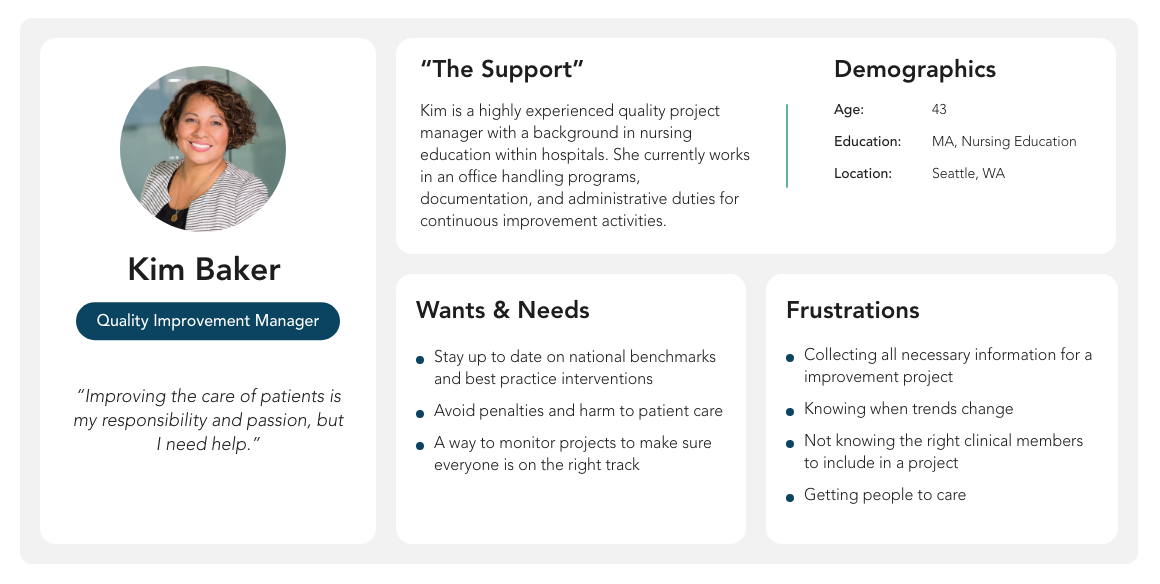
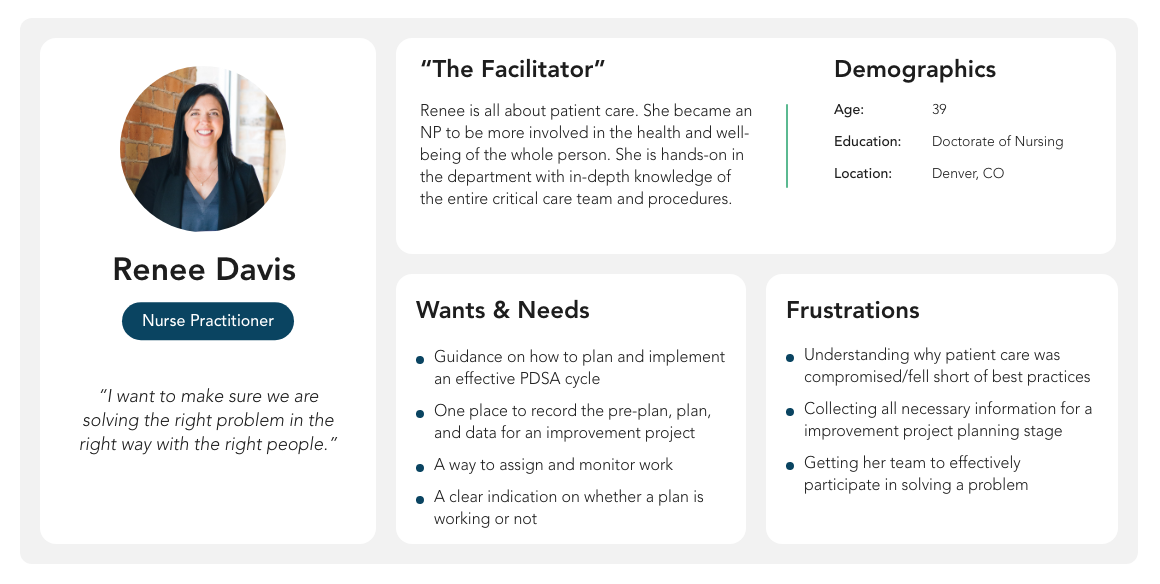
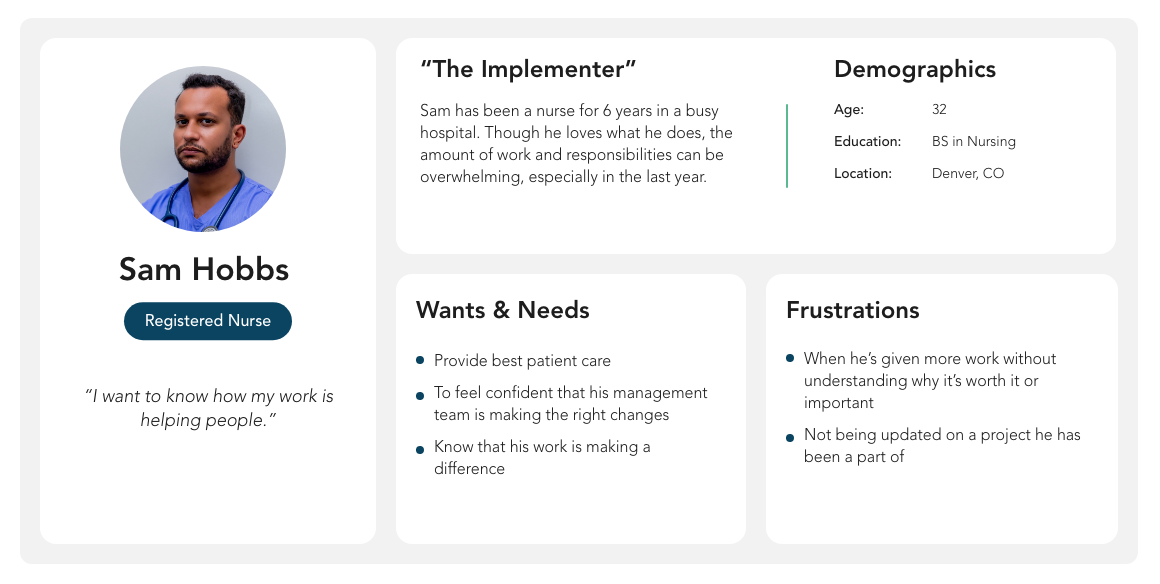
With our SME, we synthesized her experience with PIP teams to build out 3 core personas.
The Support: In every project, there needs to be administrative support. This can commonly be the Quality Manager, but their role is not necessarily medical. They are in offices working with departments on quality efforts, and reporting back to corporate.
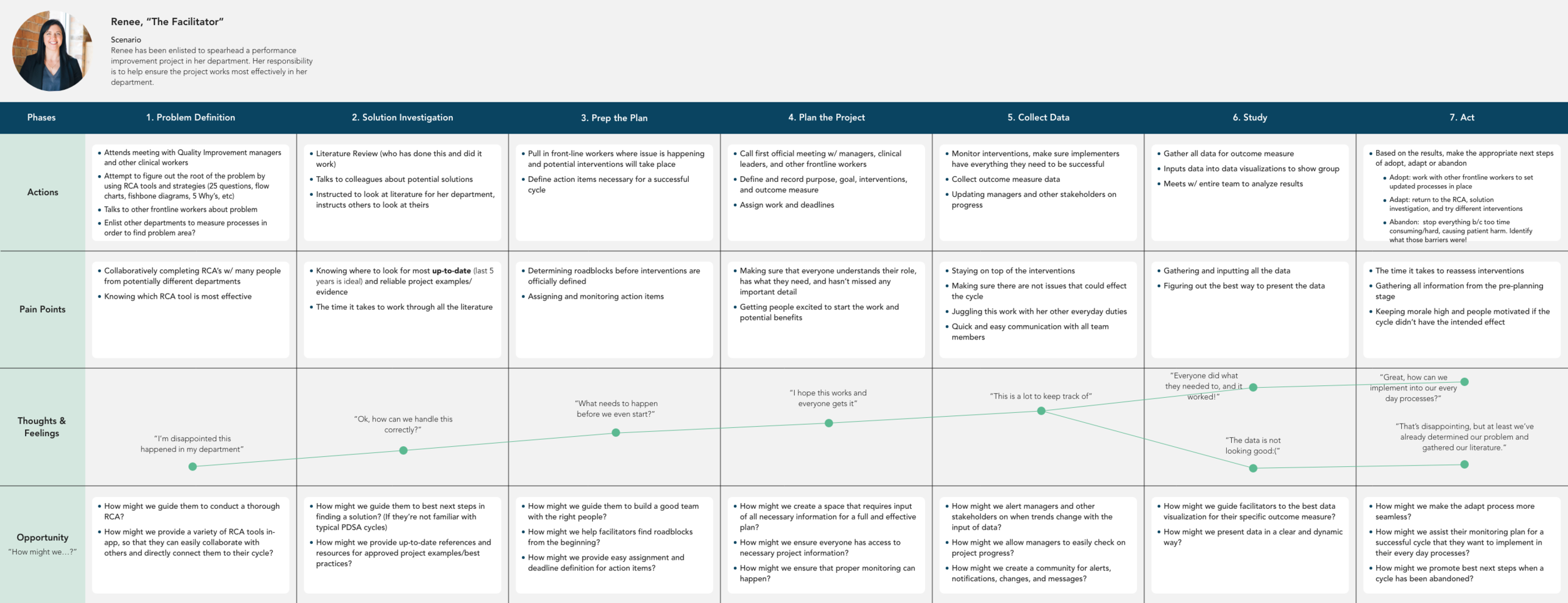
The Facilitator: This is the person who is actually facilitating the project, and they are commonly a front-line worker who is more familiar with the department’s current processes and employees.
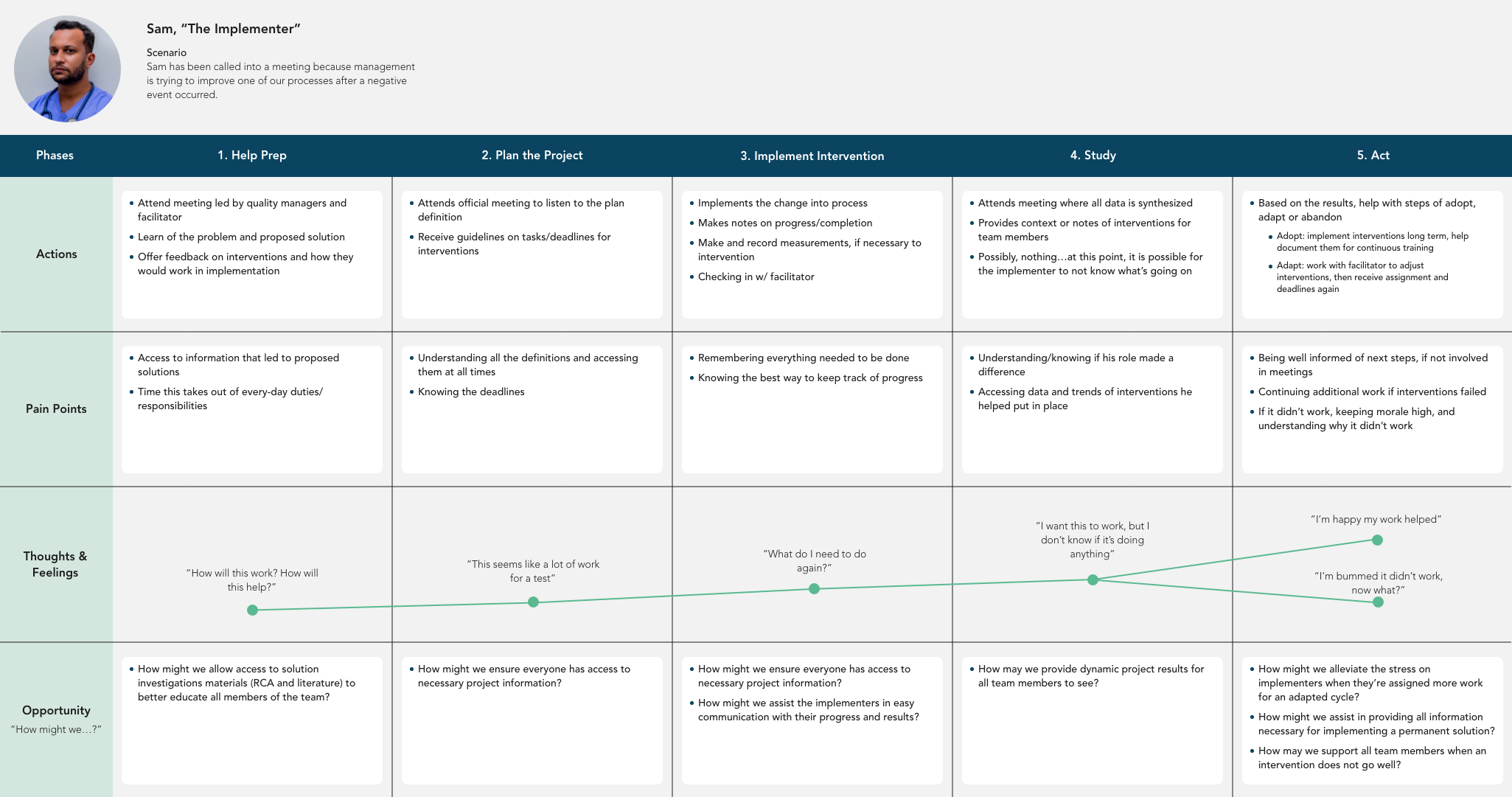
The Implementor: This is the team member who is implementing changes to processes and reporting back to their facilitator.
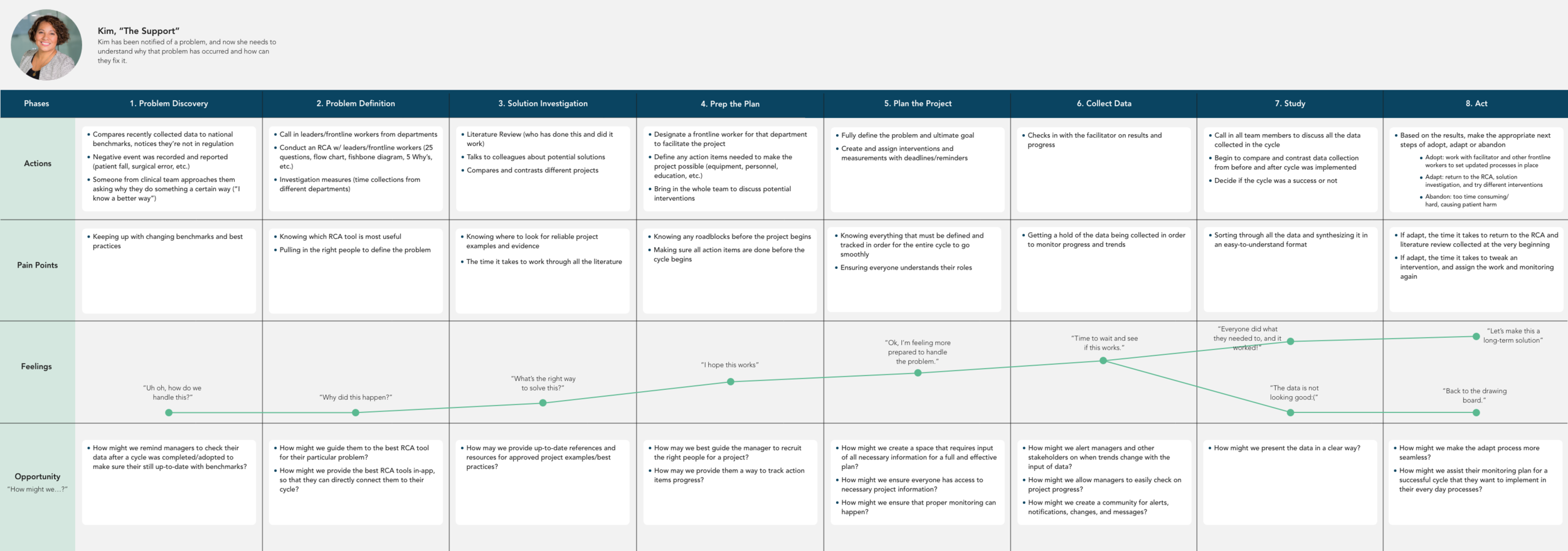
Journey Mapping
As this is a step-by-step experience, it was important for us to understand the journey that each persona went through when conducting a PIP. Basically, what is their current experience when conducting a PDSA cycle, and how can a product be beneficial at each one of those points?
Process mapping and context scenarios
After working through the personas and journey maps, we felt comfortable understanding who we were designing for and what they needed, but we still needed to bridge the gap between all of our synthesized research and design. The journey maps carefully mapped out what the process of a PDSA cycle without a product, but how would those processes change with abaqis involved? How could a product be used in these real-world situations?
Process Map

Mapping out the process of a performance project was a crucial step to our discovery because it began to incorporate phases that were outside of the actual PIP. This showed us that there can be different feature touch points depending on the user’s understanding of the problem presented to them. This led us to begin thinking about other tools that can be connected to a performance improvement project: a Root Cause Analysis Tool and Plan of Correction.
At this point, our Product Owner and Manager decided that we will explore those additional features, but the first release will be an enhanced PIP tool. We continued our discovery into PIPs using the PDSA cycle through context scenarios.
Context Scenarios
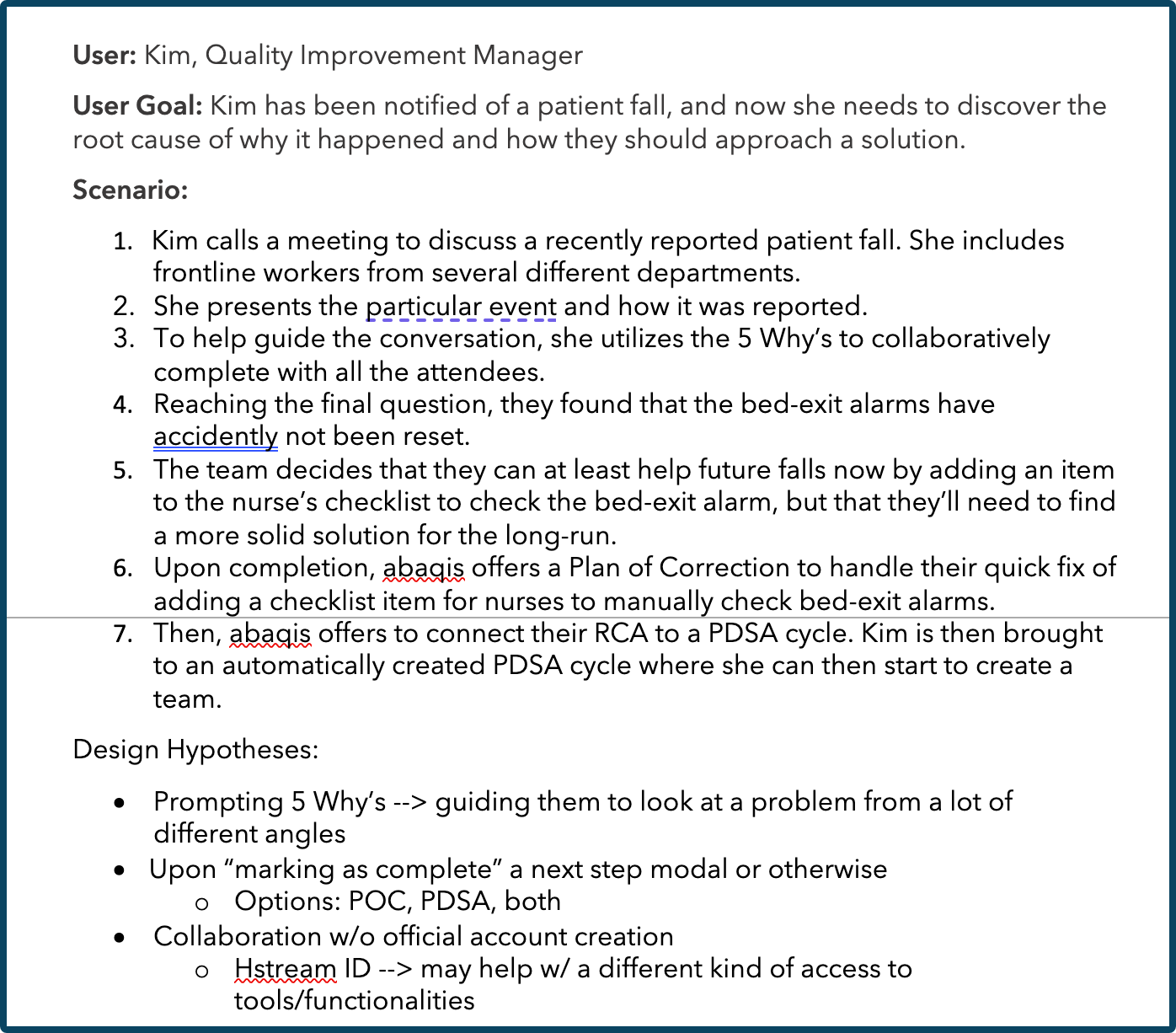
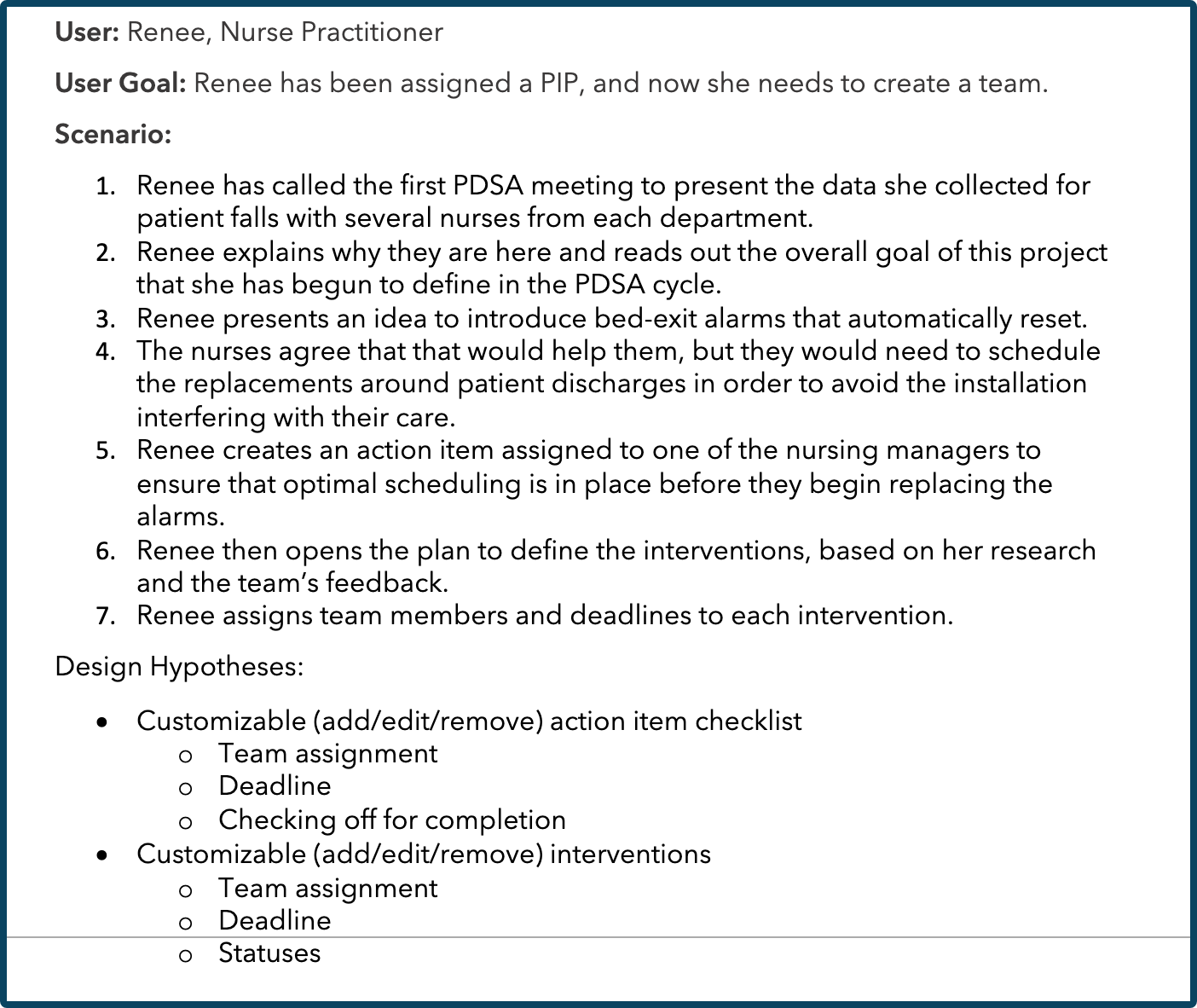
DESIGNS
Wireframes
Iteration #1: Layout and initial content


This was the first ideation phase we went through, and the major stakeholder feedback we received was that we needed to remove such focus from secondary pieces of the page such as Team, Supporting Docs, and Meeting Minutes. Those were important, but the focus should truly be on the interventions created and their corresponding measurements.
Iteration #2:

With Team, Supporting Docs, and Activity Log taking a secondary place on the page, we gave more focus to the Interventions. It is also at this point we wanted to add “Action Items”, which we learned from our SME, as well as post-acute care professionals, that there are efforts that must be completed before interventions start so as prevent any unintended consequences for patients.
As we were working through this iteration with stakeholders, including one of our trainers and sales managers who used to work in nursing homes, we received feedback that this iteration was lacking the guidance that we found was so important for inexperienced users to complete a successful project. How do they know where to start? How will they know the best way to perform each step?
Iteration #3:


At this point, we redesigned the way the core pieces of the project were displayed. In this iteration, we were able to present the steps in the order in which they should be completed. We also were able to provide a space for best practice guidance for each one of these steps, so that inexperienced users can feel confident in their work.
Stakeholders were more pleased with this version because it created a more step-by-step process for users to follow, and it uses a component structure similar to other features we have in abaqis. This structure will be familiar to current users, and developer’s will be able to use the already built architecture.
MOVING FORWARD
This project is ongoing, and we are still at the ideation stage using low-fidelity wireframes to develop each step of the PIP process, as well as management around creation, team assignment, and intervention creation, editing, and deleting.
Next steps will be to refine wireframes for early testing with existing abaqis users and potential users in the acute care setting.